
Exchange of messages by email and on Facebook are reflected upon here.
Jump to Essay 293 for graphs.
I see three categories for consideration in the context of the coronavirus outbreak, Covid-19, often called 'the novel coronavirus'. ¹
i) Understanding the medical bits.
I've put some explanation of how a virus is named down below, but we need to be clear that the virus is SARS-CoV-2 while the disease it causes is Covid-19. What you do to avoid infection is, basically, keep yourself clean —loads of washing and stay away from contamination. Assuming the continued spread of the disease, including the likelihood that the pandemic becomes endemic (i.e. it spreads across the globe and then becomes largely normal, perpetuating within the population), I list things that have occurred to me as likely events.
ii) Changes in our society, including what you might prefer to think of as cultural changes.
iii) Economic effects.
_____________________
(i) Medical
Looking at the disease and its spread, we have a collection of difficulties. Trying to model the spread of a disease soon causes one to recognise some of these: when does an infected person show symptoms? When does an infected person become infectious? What is the time from infection to being ill, called incubation period? Once ill, what is the survival rate? Is there long-term damage? Are there any preventatives (and are the carers at risk)? If you didn't catch it, are you immune? If you've recovered, are you immune? Does this target specific sub-groups in the population?
We have some answers, but many of these questions persevere, because it is quite possible to have the illness only mildly—your system deals with it. Incubation period is thought to be 7-14 days, but there are exceptions already. We are really uncertain about infectiousness. The death rate is around 1-3% but there are counting issues, discussed below. It appears to target those already with an underlying issue, those whose immune systems are relatively weak; unusually, that does not include the young, so the illness is in some senses targeting the elderly. I found a report that said someone had caught the disease a second time. This is considered unlikely. ⁵
For consideration of the speed of the outbreak, see my modelling commentary from that last week of Jan, externally or internally elsewhere on this site. The first hint that China's actions had an effect was 29th Jan.
Noted points, some of which iterate content above:
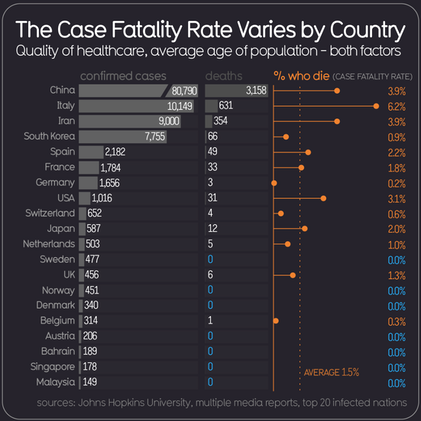
A counting problem: it is easiest to count only hospitalised cases and to use that as a test for inclusion in figures. The very many mild cases fail to reach countable status. We have the same problem with other influenzas and viral outbreaks. So any figure representing a fatality rate, such as deaths / cases is skewed heavily if a load of people have it or have had it and are not recorded as such. In turn that means that 'cases' becomes 'cases we know about'.
Information on the genome of the disease was shared very quickly; Nature published an article on 4Feb2020 [2].
A containment problem: we've known about diffusion of diseases a very long time. The diffusion rate of the Black Death was slightly faster than a hurried horse and the reasoning has not changed at all. People are amazingly selfish when faced with a threat, especially an unseen one. "The needs of the many outweigh those of the few."²
This disease attacks those with underlying problems. Most viruses attack those with weak immune systems, but this one does not target the young (as is usual). That makes it one to note as functioning in combination with other problems.
It is difficult to compare this with other outbreaks since we are pretty good at vaccination, especially in the UK. However the lead time for a vaccine is high; the design(s) is/are done already, but the slow bit is human testing, itself much of a year. Licensing a vaccine is another game entirely. "The first vaccine for any of these emerging disease vaccines like SARS, Ebola, pandemic flu, are licensed in a four year period.” Source. A typical time from design to 'ready' is six or seven months. Without the testing.
Apparently, Britain has no in-country facilities for generating vaccine stock. So that is poor security of supply, which is something we will see criticised around the world as the year goes by. See link (in the line above) for comment on public sector vaccine manufacturing. We can make anthrax vaccine in the UK, but that's it. Different topic, left to be explored by others. Suffice it to say that the thinking is that the market, meaning pharmaceutical suppliers, has this well-covered. True, but at what cost? Could a nation do better?
There are issues with this sort of disease: one can be infectious but not exhibit symptoms, i.e. be asymptomatic. Perhaps one can catch it a second time, which makes survival not meaning immune. Diagnostic testing is difficult, when it needs to be early, quick, reliable and cheap. Thus spread is inevitable, which is why 'containment' was always a short-term strategy and 'delay' is necessary but difficult.
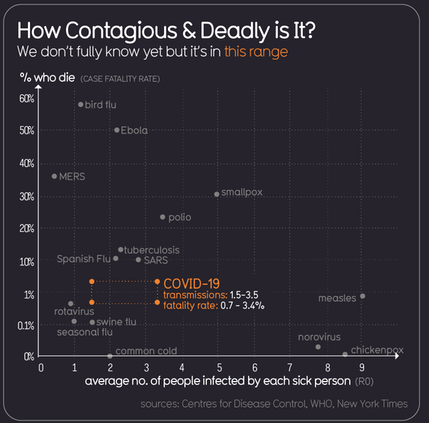
The death rate of those hospitalised is around 9%, but that is also true for HxNx viruses, even in Britain.³ The death rate at the moment is declared to be 1.4% but could be 3% — the counting problem gets in the way and so what is counted is all 'tested' deaths and all those tested positive, i.e., counting only people certain to have had the disease. That is not all who have been sick, nor is it who have had this infection. So we should recognise that there are many viruses and many of these are bad news; it is just this one that is sweeping across the world right now, but it is adding to the existing level of disease spread, so we shouldn't treat it as the sole cause of our problems.
We could easily reach a point where 40±20% of adults will catch this. That puts the death toll worldwide in the tens of millions, if we stick with current rates. I noted two weeks ago that a rate of 1% death means it is very likely every one of us will personally know someone who died from this by this date next year. At 3% that will include most people's extended families. That is nothing like bubonic plague, but it really is not good. Thanos would disagree.⁴
The targeted older folk (they are more susceptible, significantly so) will have tremendous consequences if this spreads as seems likely. Evidence at the end of March suggests that the mortality rate of those who reach hospital is largely independent of age; that is, while elderly people are more susceptible, if this hits a much younger person badly enough to be admitted then the mortality is pretty similar. No doubt better figures will appear in time, but meanwhile we have the perennial problem of bad information mixed in with the good, e.g. one of my neighbours believes that the mortality is 80% male, 20% female. Edit 20200405: I eventually found that 70:30 is apparently correct. ⁶
Social changes:
Forms of greeting need to change. Gone soon, the handshake; hugging & kissing of all but the closest family; many Continental habits need extreme change. I suggest a little bow will return.
Social gatherings may well significantly reduce. I predicted the crowd reduction actions weeks ago, but the same thinking applies to church (you're kidding about sharing the chalice, right? No more mutual "sharing of the peace"). What about all those little clubs, like choir, drama, etc etc? Changing rooms may become a thing of the past, or instead we may need to develop a whole new approach to mingling, like the two metre separation discussed in the press last week. In China, where crowds are in physical contact, such is the density, this is as yet impossible to understand; they could have a decimation (losing a tenth of the population).
Globally this level of loss is a good thing, losing a dramatic fraction of the population. At any personal level it will be a disaster.
This could be the making of the internet, but we need, very rapidly, all sorts of proof of trustworthiness (and we've needed them for years already).
The perceived social pressure to reduce travelling is going to increase and to harden into regulation. That will be a disaster for tourism (it'll move online, to become (even) more like voyeurism) and will affect all sorts of locomotion, but particularly difficult for public transportation. Indeed I see a need for certified cleaning — 'this <vehicle, rentable space> is safe and certified clean since the last <user>'.
Delivery services are going to boom. Self-isolation works if deliveries avoid physical contact. Ideally the delivery is 'clean' not just for the driver but for the received goods. Can a virus be zapped with heat or UV? Apparently so: Feb 2018; imagine the house doorway including a UVC zapper; all buildings in general, actually, but that would only be a supplementary action.
Conversely, I think shopping is going to suffer hugely; look at the way so many people handle everything they 'look' at; that has to change overnight and many will simply stay away, because Joe Public simply cannot be trusted to do anything correctly. There'll be a surge in remote telling (self-service tills) and in screens where staffing of the POS is required — difficult; I can't envisage how B&Q or Zara will function, though I have little difficulty with Tesco and Boots. The campaign to reduce the use of single-use plastics is about to take a severe knock. All sorts of official visitors are going to have an immediate and significant problem, which might move dramatically, such that the issue becomes one for the maintenance worker —for example, my gas meter is read remotely but it has to be maintained by a different sort of worker with fewer visits.
The threshold at which being ill means one does not go to work has to change (is changing already) and this could be a good thing; it depends how employers are encouraged to view the situation. That might well change how we view Sick Pay. I think every employer is going to need to find partial occupation for every member of staff that can be done away from site, though I also see lots of opportunity for job sharing ("I'm provably well this week, so I'm on the 'available' list for <anything requiring mixing with people, including shelf-stacking>; "I'm in self-isolation this week, so I can't do <list> but I can do <list>". These require very high levels of co-operation, quite likely including a dramatic change in the value of certain jobs to society; we could have something amounting to danger money for what at the moment are seen as low-quality tasks. So what has been called a sick day might morph into an at-home day, protecting the other, presumed well, staff and at the same time dealing with the presenteeism that causes so many to be not entirely well so very often.
Education might well change overnight, as it has already in China, where my friends still out there have already been teaching via the internet. How long before courses are run at the speed of the off-site student? How does examination remain secure? How does the role of the teacher change? Is there an interim state for those who cannot stay at home during school time? Already my daughter (tertiary sector) is (re-) discovering ways to get around the perceived need for shared time (i.e. doing it face-to-face but not in the same physical room); teaching could change quite a lot and I see it becoming far more student-led; the big problem there is how to 'get at' those determined to slide out at the bottom, but that is something we have generally refused to tackle for generations.
We have a significant change coming in attitude to bio-hazards; how we perceive them, what is acceptable action, what is within regulation, etc, etc.
Ability to stay clean at the new high level of acceptability is going to demand all sorts of change in public spaces. We may have everyone wearing masks outside — with consequential increases in failure to be recognised, failure to communicate, multiple ways of breakdown of society; all of this is to be avoided if we are to keep our society recognisable. We could see a dramatic failure in public trust, worse than we have already. That said, I can see why this same feature encourages localisation and hence Fear of the Stranger. Hence, I repeat, we need certification of appropriate cleanliness.
Migration will be even more in demand and even more fought against.
Economic matters
A general economic slowdown has been obvious since the outbreak and I'd expected changes to be visible at the end of January.
Looking at effects on the economy, starting from effects generated above:
Tourism takes a big hit; that's venues, localities, service providers, the works. Airlines ditto. Cornwall goes backwards 50 years — or becomes a safe haven of a backwater, which is how I'd see it. Travelling for leisure could become a thing of the past. What would that do to National Parks? Eden? National Trust? Repetition here.
The hotel business as a whole might damn near morph into a quite different sort of accommodation service. Such as a way-house for those in isolation.
Delivery services could change into something really positive.
All national transport services need a dramatic re-think. And we haven't any capital reserves for that.
The demand for nationwide internet coverage to be 100% already exists, This is already too late; if we had it, there would be a move by some to live at a greater separation than at the moment. The demand for personal (safe) space might well fuel a different demand for bigger houses or a different (lower? less uneven? Investigate) density of living. Maybe we will have people looking at regulation for that, too. However, it needs saying; we suddenly need for all internet services to be fully delivered and amazingly reliable.
The health services have a whole new ball-game. Issues about national security of supply need revisiting (they always do, but we're very bad at reporting on this); my son reports that this is quite different in NZ, but he may be in a privileged position of knowledge, having been at one time partially responsible for such matters.
Adjustments on the stock market were anticipated among my regular correspondents. What we have seen so far is but a beginning and I see this all too easily getting right out of hand. Given that the sector exhibits a lot of herd behaviour (what the wife calls herd community), it'll get a lot worse before settling somewhere better than the most extreme drop. If everyone's money were to fall in value equally it'd make no difference — but we know it won't, even if we cannot predict how things will fall out. No doubt the extremes will become more so (the rich richer, etc) and opportunists will thrive. I've seen people getting in on the demand for sanitiser with targeted scams already reported — opportunity is a sword with at least two edges.
There's a secondary, different 'hit' at the stock market to include: loads of people in close physical proximity.
The campaign to 'delay' spread of disease is going to hit all business in the short term, such is our insistence on face-to-face dealing. That has to change very rapidly and those who survive are, as ever, the most flexible.
"Adapt and survive" applies.
I've made some charts and put these on page 293.
DJS 20200310
All the charts with a black background are from source [6]. Do visit that site and my charts in essay 293 for an updated position.
Edit 20200405 I uploaded my first two pages on this general topic, Epidemics and Coronavirus at the end of January. Two weeks after uploading this page I moved what was previously below and on this page to its own page, calling it essay 293 and updating those daily while the outbreak justified such action. By early April, many of my predictions have already been evidenced, though no doubt the end result of any of these will be different from my conception.
Edit 20200528 Small matters like verb agreements and plurals changed, but nothing substantive. From the perspective of late May this has been a traumatic two months and, moving into week 11, the page above reads as precscient. Some of the things I thought would happen have already occurred; the press is beginning to catch up with topics that need to be explored. As yet no-one has openly discussed (in ways that I find, anyway) matter such as trust, certification and proof. Transparency from the state is so bad I wrote about that separately.
Edit 20200628 Struck all over again at the end of June how prophetic this has proved. I have not edited this in the sense of subtracting or adding a paragraph c/o hindsight; my dyslexic fingers typed not edited but e-tidied, which would be accidentally accurate.
[1] http://theconversation.com/h1n1-h5n1-h7n9-what-on-earth-does-it-all-mean-14815
[2] https://theconversation.com/is-it-really-the-flu-the-other-viruses-making-you-ill-in-winter-14895
[3] https://www.nature.com/articles/s41564-020-0695-z Note this published February 2019; that's very quick.
[4] https://en.wikipedia.org/wiki/Bubonic_plague The usual high standard. Yes, I made my contribution at Christmas. In 1347, the start of the second extended outbreak, Europe lost about a third of its population. See also [5]
[5] http://thebritishgeographer.weebly.com/the-spread-of-disease-and-its-management.html
[6] https://informationisbeautiful.net and https://informationisbeautiful.net/visualizations/covid-19-coronavirus-infographic-datapack/
.... though essay 293 favours worldometers as the prime source of collected data.
[7] https://www.facebook.com/dataisbeautifull/?ref=page_internal
1 It's novel because it is a 'new' coronavirus; there are many, like dozens. Wrong: it's novel because it came from animals and that is what makes it 'new', new to humans.
2 Spock, Star Trek II: The Wrath of Khan, 2015. Spock says, “Logic clearly dictates that the needs of the many outweigh the needs of the few.” Captain Kirk answers, “Or the one.” source
3 I first wrote other HnNn viruses, but that is wrong, since coronavirus is NOT an influenza-type A virus.
HⁿNⁿ explained: H=haemagglutinin, N= Neuraminidase. H and N are spikes on the surface of a spherical virus.
4 Thanos would disagree. Avengers: Infinity War (2018) Thanos sees humankind as an infestation and one that needs a dramatic culling. Whether this is a reduction to 10% or 1% or 0% of its levels at the time is mayhap a subjective understanding of the plot. My understanding was to a non-zero but low level; the missus says zero was the target. See https://en.wikipedia.org/wiki/Thanos
5 Edit end of March: medical staff 'on the front line', i.e. dealing with the ill and very ill, are subject to a high 'viral load'; this means that the amount of virus getting into their bodies has very much more chance of causing significant illness. Hence the significant need to preserve these people, to keep them available to work with the ill. So it is not that the health workers are in any sense weak, but that their bodies are being attacked far more than, say, me, in general isolation most of the time just by virtue of being retired and in the house on my own most days. The frontline workers are in an environment with a lot of virus around, a very much greater opportunity for the virus to cross their skin boundary and, when that happens, for there to be a lot more volume of virus for the body to deal with. Unsurprisingly then, the medics get sick, even when they are careful. So 'protect the NHS' makes a lot of sense.
6 Edit, end of March; it would appear that deaths do lean towards the male, maybe 70:30. report, better report
Addenda, written at the time, 20200310:
For what is called influenza A, there are 17 types of H and 9 of N, suggesting 17x9 = 153 different possibilities. Most Infl-A infect birds, some pigs; H7N9 (China, 2013) didn't affect birds but killed about a third of the infected humans. The 1918 pandemic and the swine flu were H1N1; the1957 Asian flu pandemic was H2N2, the 1968 Hong Kong pandemic was H3N2. Currently in circulation are H1N1 and H3N2. H5N1 and H7N9 directly infect humans from birds but (as yet) have not mutated to transfer human-to-human.
Influenza type B doesn't circulate in animals (so, apparently, that means they can't cause a pandemic).
"Flu shots" are vaccines made from selected strains in circulation at the end of spring, delivered (in Britain) in October and November of the same year. Source [1].
I discover (end of March) that 'flu A and 'flu B are anticipated at opposite ends of the 'season', late autumn round to early spring. Influenza C mainly occurs in humans, but has been known to also occur in dogs and pigs. Influenza D is found mainly in cattle. According to the Centers for Disease Control and Prevention (CDC) Trusted Source, it’s not known to infect or cause illness in humans. Source. What works for A&B (zanamivir, oseltamivir, and peramivir medications) by reducing the ability of the virus to release itself from infected cells is ineffective in treating illness caused by influenza C.
That last source, healthline, also says that the seasonal influenza infections A&B divide 75%:25% for A:B.
Just because you have a virus, doesn't make it the flu. [2] Coronaviruses are one such and include MERS and SARS (2003, more deadly but less infectious than Covid-19). Antibiotics don't work on viruses, antibiotics work on only bacteria. HIV is a virus. Measles is caused by the virus rubeola. Properly Covid-19 is the disease previously called 'the novel 2019 coronavirus' and its virus is 'the Covid-19 virus'. It, the virus, is also called SARS-CoV-2, because it is indeed a severe acute respiratory syndrome relation and both are coronaviruses. Distinctions are made between the disease (WHO, CoVid-19), the virus (virologists) and the species (ICTV, SARS-CoV-2) [3].
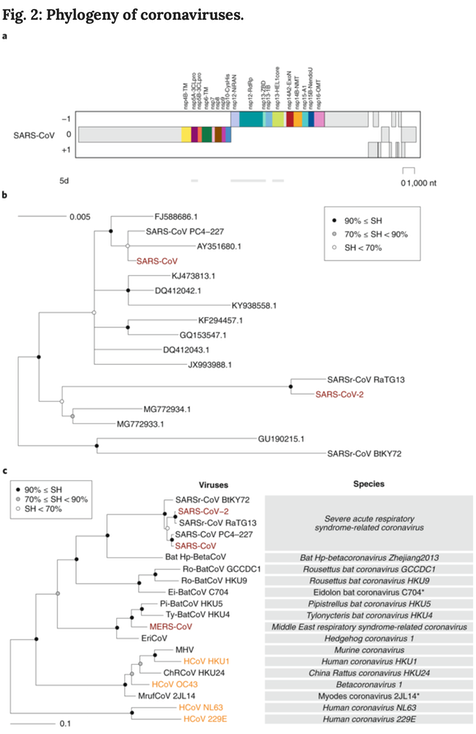
The current classification of coronaviruses recognizes 39 species in 27 subgenera, five genera and two subfamilies that belong to the family Coronaviridae, suborder Cornidovirineae, order Nidovirales and realm Riboviria17,18,19 (Fig. 1, to the right, see [3]). The situation with SARS-CoV-2 is fundamentally different because this virus is assigned to an existing species that contains hundreds of known viruses predominantly isolated from humans and diverse bats. All these viruses have names derived from SARS-CoV, although only the human isolates collected during the 2002–2003 outbreak have been confirmed to cause SARS in infected individuals. [3]
Having now established different names for the causative virus (SARS-CoV-2) and the disease (COVID-19), the CSG hopes that this will raise awareness in both the general public and public health authorities regarding the difference between these two entities. The CSG promotes this clear distinction because it will help improve the outbreak management and also reduces the risk of confusing virus and disease, as has been the case over many years with SARS-CoV (the virus) and SARS (the disease). [3]
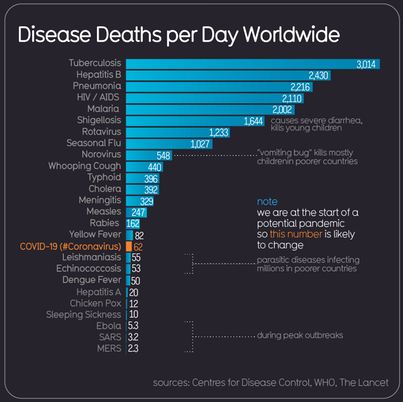
SARS-CoV and SARS-CoV-2 are very similar, but one is not a descendant of the other — that is, the diseases developed independently. The source virus is commonly found in bats, so a description that says it developed from bats has validity, but saying that the disease came directly from bats is not true; the virus may have done. Civets (cat, not bat) also have been a source of a similar virus in the past. Source [3] indicates that a new naming system is needed. Source [6] shows relative sizes of deaths due to disease, adjacent. This tells us it is the newness we're agitating about; as [6] puts it, media mentions (in millions) for recent outbreaks have been, up to today: SARS 56, HIV 40, MERS 23, Ebola 11, — and Covid-19 / coronavirus a whopping 1100. That may say more about the ways in which we have changed the way we use the internet than how we think about disease.
I like source [6] and found a similar site, data is beautiful [7], which doesn't seem to be anywhere but the facebook platform. [7] shows a collection of timelapse charts relevant to this topic.
DJS 20200313
I am amazed at the extent to which HM.gov came to such very similar conclusions. Re-reading this towards the end of March, only ten days later, we have already seen many of these predictions above occur. A fast moving position. I moved, today, the several graphs and charts that I built and maintain to a new page. Some further small edits done on the last day of March, adding two footnotes made from subsequent discoveries or realisations. Not uploaded until April1, but no foolery intended. Links to later pages are obvious additions
Related Pages:
Essay 291 - Effects of an outbreak what it says, effects, but some description of what we have (and not)
Essay 293 - Covid-19 charts charts published daily reflecting concerns and issues.
Essay 295 Long-term Distancing
Coronavirus (Y10+) modelling problems
Epidemics more general theory
Infectious disease looking at the 2020 problem, particularly effects of the reproduction number changing.
Essay 298 Covid Consequences surprisingly prescient, considering when it was written.
Essay 304 Covid Disparities A report on the report, including what it doesn't say.
Viruses are very small Worth reading, I think. (But I would, wouldn't I?)
Essay 318 Covid in October charts updated through November
Longer term issues (April 2nd):
Yes, we might well rethink working from home, which, as I have written on here, might have consequences for the size of your home—to include office space previously offsite—and the space around your home, but there are longer term consequences. Reading CityLab, I am reminded that the Victorian sewage system of which London has been so proud was in part a reaction to disease. So when we rethink globalisation we might also rethink urbanisation, moving instead to forms of localisation. But, as I've alredy written, that might too easily encourage fear of the foreigner, a Bad Thing.
I note that the countries hard hit by SARS in 2003 are the same countries that have flattened the curve, as the saying now has it, more effectively (faster, harder, more thoroughly) than other nations. They have done this with a raft of measures, but significantly more and more immediate co-operation from the public. The widespread use of technology (do see here) and the acceptance of public information (example, slow to load; I mean your information being made public) and immediate enforcement are things which 'the west' will fight against as a loss of 'rights'. That implies some deeper thinking about what society stands for and how we go about maintaining it. Localisation also means decentralisation: the UK might well do devolvement more thoroughly (i.e., apply it to bits of England) and for many that would be very welcome. At the same time we may recognise a need to decentralise all sorts of things like hospitals. Do read my ideas on the 15 minute city as a possible response. I think many will dive for the opportunity to use internet-based solutions, but that also requires that it be remarkably secure and reliable, and that the many opportunities for malfeasance are stamped out (or at the least, enthusiastically stamped upon).
One of those issues, if we seek localisation, is that we may well lose (just perhaps, change / rethink) the benefits of mingling physically with other people. I am far from certain what these benefits are, but I read often about the synergy of proximity, how it is that ideas develop from people non-deliberately mixing. I think we could move that to the internet, especially if we could dampen the echo-chamber effect—so that any individual is confronted with more different responses rather than reflections of their own declared attitudes. The sort of thing that editorial comment on a newspaper piece generates (but is actually controlled by editors). Something as simple as resetting the social media algorithms; imagine if an individual not only had a financial risk setting, but a social media risk setting—the risk of reading a dissenting opinion.
I wonder how many (even which) temporary regulations will oh-so-slowly be removed by various governments. I wonder about knock-on effects; for example, if travel reduces dramatically, does that mean that road maintenance becomes rediverted to local routes rather than trunk routes? Would significant decentralisation make regions of Britain as different as US states? Would that be a bad thing? What systems would we (all) agree needed to remain centralised, and might that no longer be automatically somewhere in the capital? Having read an awful lot of s-f, when will people try using avatars (in volume) and what will be done to make that not-happen? When can I have a proven signature, what we require as evidence that the 'me' responding electronically is the 'real' me; further, how do we protect that position from abuse?
When communications are bad, crime is difficult and localised;
When communications are good, crime is easy;
When communications are perfect, crime is very difficult.
I failed to find the quote: this is what I remember from the mid-60s. That's 1960s, not my mid-60s.
Related pages:
Essay 291 - Effects of an outbreak what it says, effects, but some description of what we have (and not)
Coronavirus (Y10+) modelling problems
Epidemics more general theory
Infectious disease looking at the 2020 problem, particularly effects of the reproduction number changing.
Viruses are very small