
The current fuss over blood clots shows up our very poor understanding of risk. The Astra Zeneca virus, after providing 20 million doses to the end of March, has produced (and possibly caused) some 79 clots of a specific type. This is equivalent to a risk of 1 in 250,000 - that four in a million might be expected to have some similar issue. Source. For the specific age-group with the minimum risk from Covid, the 20-29 age group, we'd expect eleven in a million to have blood clots over a period of, I think, 16 weeks. Vaccinating a million 20-29 age people would save 8 from intensive care with Covid. Eleven is slightly larger than eight, so for this group the 'risk of clots' is bigger than the 'risk of covid'. But both of these are very small and we ought to put these in context with other things we simply accept as entirely normal.
For the relatively young it might be better to use a different vaccine. But one observes that we don't have the same sort of volume of vaccinations, nor the study time, to know what (bad) effects other vaccines might have. There is an unsupported presumption that whatever those are, they're different and smaller still. One example chosen by talking heads is the contraceptive pill, which has a possibility of producing blood clots (picked for being much the same result) quite a bit higher than from the A-Z vaccine; about 500 per million women per year in the UK (see) and twice that in the US. Deep vein thrombosis—basically, blood clots—runs at about 1000 per million per year in Britain and is vastly increased by long-distance air travel, and by major surgery such as joint reconstruction, for which there is a lot of data.
David Spiegelhalter has written briefly about this, after my first draft, here. He uses the unit which I'm calling phut, per hundred thousand. The incidence of blood clots linked to having had the A-Z vaccine is one phut (my figure above says less, 40% of that, but he's using the EMA figure. ¹ The similar activities I was hoping he would give us are included, as (i) dying from general anaesthesia and (ii) a single skydiving jump. ² He too uses the Pill comparison.
What I find curious about this situation is that even reporters trying to be balanced manage to pass on some level of 'you want to avoid this', when the figures say that being struck by lightning is about 0.8 per million (and you have to be outside for that to happen, surely?), while the risk of death from car accident in the UK is about 59 per million each year. (source, google, basically) – and the UK has very much better figures in this regard than you might think.
___________________
Relative risk: that being the risk of my relatives bumping me off from telling bad jokes and bad jokes badly. Or it could be the risk to my relatives for being associated with me.
____________________
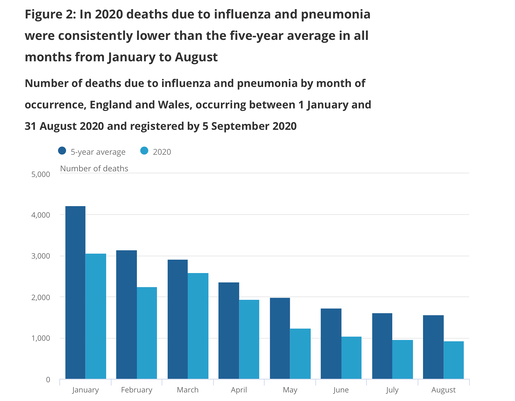
Still on covid, though from a different aspect, one notes that death fron the 'flu is way down for the last two winters. Which I read as being an encouragement for "hands, face, space" to continue. Deaths from 'flu in Britain run at around 20,000 per year even though we vaccinate against this. There is a surfeit of available information and I have had difficulty finding useful trend figures. Try this, and its figure 2, copied here ---->. One could argue that the people who would have caught 'flu instead caught covid (and many more died as a result); one can argue that we've lost a load of people susceptible to such illness earlier than we would otherwise have expected, so we might argue that the 'flu-related deaths will be depressed for the next few years. Of course, we might also have learned a few things and adjust individual and even collective behaviour to further suppress diseases of this sort.
Most of this, like my first topic, centres around recognition of relative risk – and whether that results in a change of behaviour. The arguments I find seem to distinguish between risks that we can mitigate—such as reading the blurb that comes with a medicine, mitigating blood clot risk on a long flight, driving with care and generally acting in recognition of risk—and those that we cannot. But I'd lump into that second 'cannot' category all those risks we have chosen not to recognise, not merely those of which we are unaware. One could easily argue that it is our own responsibility to be aware of risks. However, how we decide where we draw the line at 'acceptable risk' is very much unclear, as is how we might discern what others do or compare with others what we think the relative risk is. Personally, I'm happy to learn what the risks are and then to attempt defences against those specific risks.
As an example, take rushing about in the hills, which has an image of being dangerous, mostly because, when the emergency services are called out, it is their interests to have publicity because, too often, this is volunteer work. Which directly means that it is their interests to advertise any event so as to raise subscription monies. In turn, that raises the perception that going into the hills is somehow 'dangerous'. In effect what we learn is that people turn the countryside into a dangerous place because they have not considered their own behaviour and so, in many ways, are a danger to themselves; indirectly they then become a danger to society at large by incurring social cost.
How might we measure the attached risk to an activity? Does experience reduce this risk or does the chosen activity move in line with the experience so that the risk is similar? Then the question becomes whether this is an activity taken by people who not only identify some attached risks but actually seek to pit themselves against such risks. This is possible, but if that is so, then those same people will be doing this manipulation of risk to their accepted level of excitement in many other spheres. The subtle difference is knowledge of what is risky. In the context of hill-walking, the lesson to learn is that abandoning a route (or a day) is a wise decision and has no attached shame—rather the reverse—and people training others in the hills might take this on board as a lesson to attempt. I remember well an occasion with a Three Peaks party where I felt it necessary to point out that for the party as a whole this was unsafe weather, but for the two leaders, alone and without the group, it was not. That would be because of experience—in a sense having been through such experiences already—and not due to having better kit (which would be quite possibly untrue). In sense the boys out on the hill had to be made aware that what we were doing was dangerous and risky enough to turn around simply because they weren't safe to be with. I've had bigger scares on boats of all sorts but am entirely aware that this is because I have less knowledge and experience about what is happening, what I might be doing wrong and in consequence I am to some extent unaware what it is that is dangerous.
____________________
Relative risk has a definition in the statistical world, where the two groups, effectively I and C in the formula to the right, do or do not act to mitigate the perceived risk.
In the safety at work sphere, one must: identify the hazards; asses the risks posed by these hazards; control the risks—which is a process in which some risks are reduced by change of process (procedure, protocol, practice); keep records; and test to see that the change has the desired effect. This compound process rather demands that you have a way of enumerating the risk attached to a (bad) result, but it turns out that evaluating this does not make the value essential. For example, if as a pedestrian you consider crossing a road, we assume that 'being hit by traffic' is a concern, so protocols would include 'looking at the traffic', but might adjust to 'use a designated crossing point' so as to reduce the attached risk. I have commented in earlier pages about applying this to being a pedestrian in China, where the traffic is permitted to turn right regardless of what the lights say, which in turn means that pedestrian crossing protection is different from the UK and that there are other moments in a traffic light cycle which are safest for a pedestrian to cross. This is a matter of testing the result of the protocol.
Best of all, of course, is to avoid the risk altogether. But that means that some twisted version of 'being safe' removes an awful lot of what we might call life activity – and, I suggest, leaves one open to risks to mental health. The population that has worked through 2020/21 has doubled, from 5% to 10%, the proportion that feels their mental health has deteriorated to the point where it needs assistance. So, to mitigate the risk of poor mental health, one ought to do some of those things with other attached risks, such as leaving one's dwelling.
Practically everything we do has attached risks, from the highly unlikely such as being hit by a meteor (which is affected by where you are only if protected by large amounts of rock-like matter, to the largely unavoidable such as what it is that is peculiar to your nation. For example, being bitten by a rabid dog is very unlikely in Britain (the only cases of rabes since 1902 are from bats) but relatively more common in Poland (8000 exposures in 2019). When any large-scale disaster occurs it is difficult to have recognised what was going to occur in time to have avoided the event. Which means that the mitigating actions require a flexibility of thought and even perhaps an acceptance of change for the worse. ³
When one chooses to do something that has known attached risks the available measure of that absolute risk is very much averaged. Deaths on the road in the UK run at around 1750 a year or around 5 deaths per billion miles travelled (source). The figures for lesser injury assume that reporting and recording occur equally across the nation and the figures tend to exclude injuries (etc) on private land. This perceived and averaged risk may affect your choice to travel at all, but it might be better to put effort into being a safer driver, which means that your perception of your safety as a consequence of your own driving is increased. You could apply the same thinking to other travel and make yourself a safer traveller. Which in turn mostly means that you recognise behaviour that threatens your safety, a lot of which is not your own behaviour. Reduction of risk is the key, here. In many cases the only way to remove a risk completely is to not do the associated activity, but once an activity is decided upon one should perhaps put some effort into attempting to avoid some risks and to reduce unavoidable risks.
So let's go back to blood clots; you're more likely to get them (link) if you:
- are staying in or recently left hospital – especially if you cannot move around much (like after an operation)
- are overweight
- smoke
- are using combined hormonal contraception such as the combined pill, contraceptive patch or vaginal ring
- have had a blood clot before
- are pregnant or have just had a baby
- have an inflammatory condition such as Crohn’s disease or rheumatoid arthritis.
These are not the only causes, but they are the most common ones.
It is perfectly clear that, if blood clots are a potential issue for you, you have quite a number of actions you could take (could have taken). Among those actions are: (i) being active, which includes not sitting still for long periods, so some minimal level of activity a lot of the time and more extreme activity every day –specifically on long-haul flights walking up and down on a per-hour basis; (ii) keeping sufficiently hydrated, which might include less coffee and a lot less alcohol; (iii) keeping your weight within a sensible range; and (iv) not smoking. All of which means that the likelihood of specifically you having a blood clot is at least partially avoidable. This is very similar, I feel, to the likelihood of having caught covid and to the possibility that, having caught it, it puts you in hospital and worse. Not everyone with blood clots nor everyone with covid is an overweight smoker who drinks heavily and takes zero exercise, but each of those labels applies less to the fit and the moderate.⁴ So while the incidence of blood clots is declared at four per million vaccinations, that does not at all mean that this risk is identical for all of us.
So there are actions we can take as individuals. But there are also actions we can take collectively. That would include all sorts of activities that make the world safer, such as 20 and 30mph zones where traffic meets pedestrians (and different rules where they don't), but also drives to reduce smoking (or the effects of smoking). Among the changes I'd like to see as part of turning the NHS into a health service rather than an illness service would be to reduce the national preponderance of obesity and to improve the general health of the nation. ⁵ We need incentives for that to occur an my page on nudges applies anew.
DJS 20210409-11
⁶ ⁷ ⁸ ⁹
1 The European medical association figure is higher for some of these possible reasons: because it's not just England; because nations are different; because counting is different. I'm not even convinced that what was counted as '79 cases to the end of March' is counting the same thing(s) as the EMA counts.
2 I have had a life insurance policy specifically excluding sky-diving. Given the risk, why are not other equivalents also excluded? I suspect that this is simply an example of avoidable risk. You most definitely choose to do a sky-dive.
3 Risk of lightning strike, 1 in 500,000 per year, two in a million (but read this). Of being struck sometime in life, 1 in 3,000 or 33 per million I still think you have to be outside at the time of the storm, which makes the chance of being hit while outside when lightning is occurring very much higher and actually what you need to know.The risk of being hit by falling objects is heavily skewed by construction site events. As for a meteor, you're more likely to win the UK lottery; David Spiegelhalter again.
4 I had a look at cycling, for which there is available data. Cycling accounts for 6% of traffic deaths and 14% of the traffic serious injuries in 2016. Just because a cyclist is a bit healthier, doesn't make them risk free, it only changes the risks. The 'fit and healthy' reduce one load of risks but generally become susceptible to a different group. The significant difference is that the overweight smoking drinker (etc) is accumulating risk that is mostly indirect, while the active person collects risk they can manage directly and therefore do quite a lot to reduce the associated risks.
5 A friend on FB posted a picture of a sunny day on the beach from 1950 - not an overweight person in sight. I've found a pair from 1950 and 2018; I don't think they make the same point.


More, 20210629. The Conversation, Geoff Mulgan, UCL. Readable, pertinent, coherent. While he points out that we had, past tense, actions in 2000 (report) these all disappeared with austerity (and Brexit, and...) such that of course we were badly prepared for a pandemic. But, as he explains, the issue is not preparation for specific events, but to have the resilience to cope with the unexpected. what we need is to be able to take risks seriously, to be able balance risks appropriately - and to be supported in making such decisions. Part of that last requires all of us to be very much better at understanding risk. I'm afraid that the political urge to be seen to Do Something, any political action at all, is so strong that most sensible actions are (have been, will be) discarded in favour of something that can be perceived as Action. Which of course, simply perpetuates the attitude to risk. Therefore it is an educational matter at root; since much of the understanding centres around understanding of probability. We need, therefore, to make this moire central to our mathematical education (but not to say that this problem lies in the teaching of mathematics and is therefore a Maths problem); we need to be able to see the applicability. if <this risk> is bigger than <that risk>, then why do we not take precautions in line with the risk? As Mulgan points out, the figures for death from slipping in the bath are high compared to being in a train crash; what we do about risk —why we do what little we do, why we persist in ignoring larger risks, how we balance different sorts of risk—remains poorly understood.
- Dying from a Heart Disease: 1 in 5
- Dying from a Cancer: 1 in 7
- Dying from a Stroke: 1 in 23
- Dying from any kind of Injury: 1 in 1,820
- Dying from Electrocution: 1 in 5,000
- Dying in a Road Accident: 1 in 8,000
- Dying from intentional Self-harm: 1 in 9,380
- Dying from an Assault: 1 in 16,421
- Being Murdered: 1 in 18,000
- Dying from a Car Accident: 1 in 18,585
- Dying from any kind of Fall: 1 in 20,666
- Dying from Accident at Work: 1 in 43,500
- Dying from Accidental Drowning: 1 in 79,065
- Dying from Exposure to Smoke, Fire, and Flames: 1 in 81,524
- Bee, Snake Venomous Sting: 1 in 100,000
- Dying from Forces of Nature (earthquake, heat, cold, lightning, flood): 1 in 225,107
- Dying from Choking on Food: 1 in 370,035
- Being Struck by Lightning: 1 in 576,000
- Drowning in a Bathtub: 1 in 685,000
- Dying from a Dog Bite: 1 in 700,000
- Fatally Slipping during a Shower: 1 in 812,232
- Dying form unintentional Alcohol Poisoning: 1 in 820,217
- Dying in a Fireworks Accident: 1 in 1,000,000
- Dying from Falling off a Ladder: 1 in 2,300,000
- Dying from Food Poisoning: 1 in 3,000,000
- Dying of a Snake Bite: 1 in 3,500,000
- Scalded by Hot Tap Water: 1 in 5,000,000
- By Falling Coconut: 1 in 250,000,000
- By a Shark Attack: 1 in 300,000,000
And odds of dying in a terrorist attack while on-board is 1 in 25,000,000 (25 million) and the overall average of dying in any kind of terrorist attack worldwide is 1 in 9,300,000 (9.3 million). Incidentally, that last iss about the same as of becoming a country's President, 1 in ten million. note that these figures are generally averaged across the world, so you might want to adjust the figures for you locality (which means where you happen to be; obviously your risk of travel death is increased if you do a lot of travelling, but perhaps the occasional traveller has different habits that change their particular risk for better or worse. For example, do you have to be outside to be struck by lightning?
What's the equivalent figure for dying in bath or shower? Since you can't do both, add the fractions; 1 in 317,605, a little more likely than from choking on food.
Do you do anything at all to mitigate these risks?
Lightning: US around 10% of those struck die, 512 cases per year this century. wiki. 240,000 events per year globally, 2000 deaths worldwide. Note that this cause of death is hard to recognise, so is probably under-reported. In the UK (source) the risk (of being struck by lightning) is 1 in 33 million (83% male) a bit under 2 per year, but half that in the last ten years. Many more people are injured (about 14 times as many, but that's still under 30 per year in the UK; as with covid, the counting is difficult).
What should you do if lightning threatens? Shelter in a building or vehicle, but there's no advantage in sheltering in an unearthed building or tree. A large part in the reduction of death from lightning is that we have earthing, so that house are safe places – through the period 1900-09, 24% of lightning deaths occurred indoors. Advised actions: BBC; low spot away from metal spikes and trees. Accuweather; away from water, tents not shelter, don't dawdle. Ramblers: lose height first (when you see it coming), lower open ground is safer than a cave or a tree (especially a lone tree), sit on insulation, move metal objects away (walking poles, tools, ice axe). NLSI: A cave is safe if a deep cave, but not if the mine has nearby metallics (e.g. old equipment). A clump of bushes or tress of uniform height is a good place, as is a ditch or trench. A bad place is an edge such as a shoreline and even being close to another person (5m spacing recommended).