
It is disturbing the extent to which we allow decision-makers to be disnumerate. Most of the problems on this page reduce eventually to comparing two numbers, recognising which is bigger and basing a putative decision upon that. This is a small part of my larger argument that a grasp of Number is much more important than Maths. Of course, I also think that anyone the slightest bit gifted with regard to maths has a very good grasp of number. But I think as a society we should insist that as close to everyone as we can manage should have a much better grasp of number than is currently evident. A large part of this decision-making issue is that the people with high technical skills seem to find it difficult to reduce the information to a point where political-level decision-makers can make sensible choices.
A long pause while I hunt for new examples. The trouble is that I'd like to use real data so that people reading this come away with real conclusions. Each time I find a likely candidate, the data slides away from actually providing a conclusion you can hang an action on.
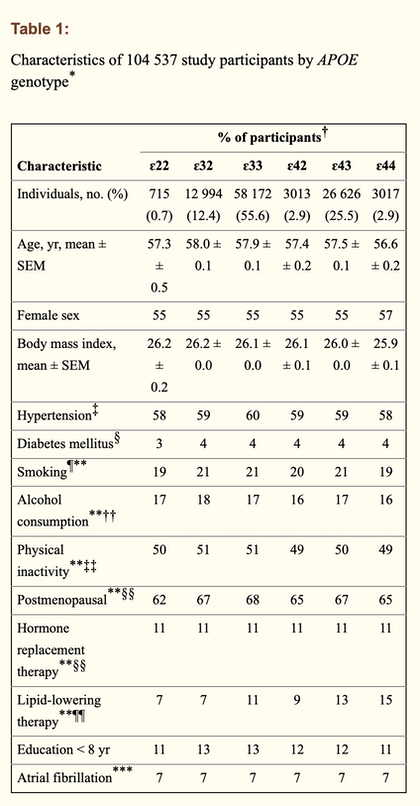
All of which led me to a study of dementia in Denmark. Among 104 537 individuals, the absolute 10-year risk of Alzheimer disease in 3017 women and men who were carriers of the APOE ɛ44 genotype was, respectively, 7% and 6% at age 60–69 years, 16% and 12% at age 70–79 years, and 24% and 19% at age 80 years and older. Corresponding values for all dementia were 10% and 8%, 22% and 19%, and 38% and 33%, respectively. Adjusted hazard ratios (HRs) for all dementia increased by genotype, from genotype ɛ22 to ɛ32 to ɛ33 to ɛ42 to ɛ43 to ɛ44 (p for trend < 0.001). Compared with ɛ33 carriers, ɛ44 carriers were more likely to develop Alzheimer disease (adjusted HR 8.74, 95% confidence interval [CI] 7.08–10.79), vascular dementia (adjusted HR 2.87, 95% CI 1.54–5.33), unspecified dementia (adjusted HR 4.68, 95% CI 3.74–5.85) and all dementia (adjusted HR 5.77, 95% CI 4.89–6.81).
The APOE ɛ44 genotype is revealed as a significant contributor, so we can with some confidence identify high-risk groups by age, gender and this genotype classification. Think of the genotype bit as expressing the genetic, heredity-based likelihood of the risk of developing dementia, but that it is the ways in which you live your life that seem to affect the likelihood on onset. This means that, if we could identify accurately those at risk—implying some threshold for action and some general advice on staying well away from the danger zone—we might significantly reduce the incidence of dementia and Alzheimer's disease.
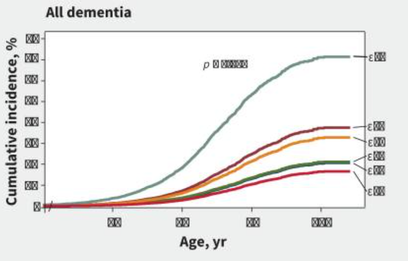
Look at Table 1. Most of the figures are percentages of the study population belonging to that category and, to my eye, are pretty consistent in each row. The particpants were examined twice at roughly ten years apart, hence the ability to express risk in the quote in brown above. The numbers developing any form of dementia increases with the genotype number, across this table. This then generates a group of graphs such as I have inset. The axes are not detailed but I imagine run from 40 or possibly 50 upwards on the x-axis stepping in tens and from 0 on the y-axis stepping in fives. The coloured lines are the genotypes in order, so the ɛ22 is the red at the bottom and the ɛ44 the top paler green. Studying the brown above we have age groups for the 60s, 70s and 80s with a gender split f/m that fits ....values for all dementia were 10% and 8%, 22% and 19%, and 38% and 33%, respectively. So whatever characteristic the ɛ44 is, it needs obvious attention. Equally, whatever the other characteristics of increasing liability for the onset of dementia as a collective term, we should all take steps to reduce them. The study quotes: Reduction of risk factors for dementia may have the potential to delay or prevent one-third of dementia cases.Link 3
Source 3, once accessed, indicates that dementia affected some 47 million over 65s globally in 2015, with this expected to triple by 2050. That seems a very low number to my mind, 0.7 % of the population, but it fits with there being 5-8% of the over 60s. WHO. The costs are estimated at $800bn, 85% of which hits the non-medical systems such as family and social care.
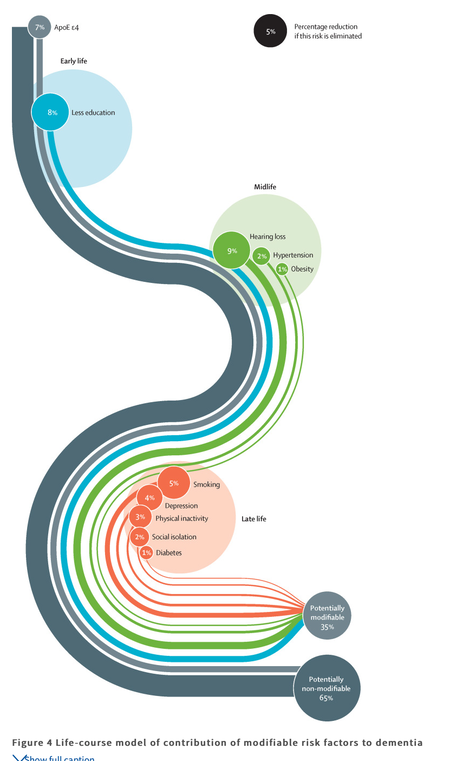
Prevention would include active treatment of hypertension in the middle aged (that's 45-65, the second half of employment), but interventions for other risk factors including more childhood education, exercise, maintaining social engagement, reducing smoking, and management of hearing loss, depression, diabetes, and obesity might have the potential to delay or prevent a third of dementia cases. Picking from the content to save you reading the whole: People with dementia often have co-morbidities; a third of older people now die with dementia; there are many different types of dementia; a delay in the onset of dementia would benefit even the oldest adults; [an] unexpected decline in age-specific dementia incidence or prevalence has been reported in some countries, [including] the USA, the UK, Sweden, the Netherlands, and Canada. US studies showed that the decrease in age-specific prevalence (despite an increase in the absolute number of people with dementia) was associated with an increase in education.
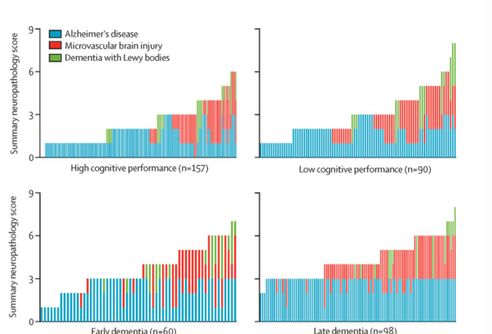
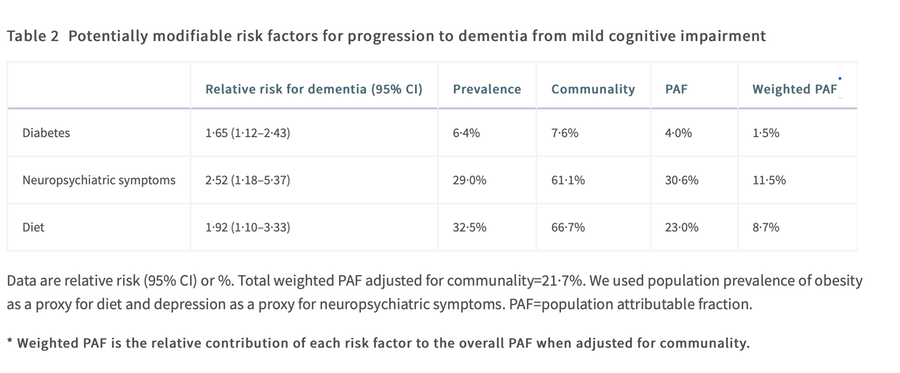
The blue and red chart set hereabouts illustrates how some individuals in community-based US studies who are cognitively healthy tolerate a large and mixed burden of vascular, Lewy body, and Alzheimer's neuropathology. These findings have led to the concept of cognitive reserve, which is that people who have such brain reserve can tolerate more neuropathology without cognitive and functional decline, and therefore develop dementia more slowly than people without this type of brain reserve. This reserve is related to either the brain anatomical substrate or adaptability of cognition, due to factors that we discuss in the next section. Which suggests that promoting this cognitive resilience and building brain reserve is a jolly good idea. This is associated quite strongly with more education (higher), better socio-economic status (notably as a child), more intellectual stimulation. All of which leads us to this table, which is followed in the paper by a lot more explanation than I give:
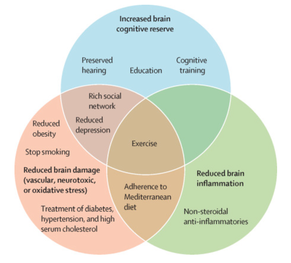
The figure at the top now becomes relevant and if you worked in the field it is the sort of thing you might print large and put on a wall. It shows the things we can do that will delay onset for the 35% or so who are reachable. The early stuff from the Danish study now makes sense of the APOE ɛ4 near the top of that diagram.
Of course, it is the usual suspects targeted as things to stop doing or better still, never have done: smoking & alcohol, inactivity, diet and obesity. But to this are added hypertension, hearing loss, depression and isolation. And do be aware of when in life this is an appreciable, adjustable factor. Detail here may be significant and I direct you to read the Lancet [3] for yourself; for example, it is when you have loss of hearing and of what type that expresses as an appreciable factor in dementia onset and progression. Exercise doesn't improve memory, but it seems to correlate with a reduction in potential losses – it has preventative value. You might look at resistance training becoming an asset in this regard. It is not clear if isolation and depression come before or after the dementia issue, nor whether these are connected to or independent of dementia. The prevention then would seem to be sufficient social contact (and we might wonder how 2020/21 has affected this).
Then there is whatever we do to improve cognition. I propose to come back to that, eventually.
DJS 20210525
1. I give in; I can't find where i started the hunt. Presumably this source flamed out, or some equivalent failure label.
2. https://alz-journals.onlinelibrary.wiley.com/doi/full/10.1002/alz.12165
APOE and dementia – resequencing and genotyping in 105,597 individuals
3 3. Livingston G, Sommerlad A, Orgeta V, et al. Dementia prevention, intervention, and care. Lancet 2017;390:2673–734.
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(17)31363-6/fulltext You may need to register to see this. No cost.
4 WHO site on dementia. https://www.who.int/news-room/fact-sheets/detail/dementia
5 https://www.businessinsider.com/population-over-60-map-2014-5?r=US&IR=T the maps are worth a look, if only for shock value.