
Looking to classify approaches to viruses, I found several versions of a classification. I've opted for there being four classes, each divided into two [1, 2]
1 Virus Vaccines
1a Live attenuated virus - a deliberate mutation of the original that pushes the body into appropriate defences.
1b Inactivated virus - disable the target virus so it doesn't replicate; inject that to generate suitable defence response.
2 Viral vector - another route to causing the body to generate antigen. E.g. adenovirus.
2a Replicating viral vector e.g. measles
2b Non-replicating viral vector, e.g. adenovirus4 Protein based vaccines
3 Nucleic acid vaccines DNA and RNA vaccines, often labelled as mRNA, contain code for a coronavirus protein so the body generates antigen.
3a DNA vaccine, uses electroporation to cross cell membrane.
3b RNA vaccine in a lipid coat to cross the cell membrane.
4 Protein-based vaccines
4a Protein subunit (of the coronavirus antigen), which won't replicate but will stimulate defence.
4b Virus-like particles -VLP- resembles coronavirus in structure but include none of the genetic material.
________________________________
A little about how they work is at [3], where not already explained by [1] and [2].
When a vaccine is developed it goes through phases of testing [4]
0. Preclinical, the plan, development, construction
1. safety, dosage small samples <100
2. effectiveness, Phase 2 trials will be 3 and 4 digit sizes
3. Phase 3 trials use large samples, typically 50k size
4. approval and licensing, subsequent monitoring
An entirely different problem is delivery. Yesterday, 20201221, I noticed for the first time a prediction that delivery within the UK to those declared at-risk for any reason is predicted to take until July, not early May as I had been thinking. That means the herd immunity point might be as far away as September or even later. In turn that might well mean that, if the fear level continues much as it has done, we lose most of 2021 to consequences of 2020. It also means that on a global scale, her immunity may be much further off, maybe 2025. I wonder if this will have consequences for global travel. IN terms of carbon reduction, that is surely a good thing.
That awful tendency of the selfish to escape any restriction and, in so doing, to cause spread—which needs a pithy label, such as escape spreading—has a parallel in climate change reduction, where people who can so afford do more travelling while that is still permitted. Of course, those in the travel industry will encourage this, their parallel being to make sales while they still are able to, but all in all this pushes nations into having to regulate towards restriction rather than have people make sensible choices and restrict themselves. That too needs a pithy label.
I recognise in myself an assumption that the coronavirus pandemic will leave that virus as endemic, not eliminated. I see this as a consequence of the diesase being viral, which, I understand, is therefore likely to mutate and often. i wonder if a viral disease can be eradicated? [8] suggests that, whtever we think of 2020, this is not 'the big one' in terms of pandemics.
DJS 20201229
30th Dec: Astra-Zeneca's vaccine AZD1222 was approved by/for the UK (NYT says for emergency use only). Moderna is (we are told) close to approval in the US; Sinopharm announces efficacy of 79% for BBIBP-CorV.
Moderna vaccine cleared for use 20210108 but won't be available until late March or April. Therefore probably discounted from calculations as not immediate enough. Probably expensive, too.
29th Jan: the growing issues between the EU and Astra-Zeneca illustrate what happens to the EU as a consequence of free movement, which has been curtailed dramatically by the pandemic. While health is a national competence (lovely phrase), the limitation of movement to prevent spread became a Union issue and somehow that meant that this stretched to the procurement of vaccines. See report. Central control would, at least in theory, benefit the less able members of the union. I suspect that ownership of the production facility will be seen as a nation-level matter – possession being the point. However, one might also look to issues of preparedness and to when a contract was made in comparison to other contracts. Of course, lawyers will disagree whether FIFO applies in accord with what supports their 'side' of the argument. Therefore I see possession being the whole of the argument. Renegotiation would seem to pragmatic solution.
[1] https://graphics.reuters.com/HEALTH-CORONAVIRUS/VACCINE/yzdpxqxnwvx/ middle school read.
[2] https://www.nature.com/articles/d41586-020-01221-y offers categories
[5] https://covid19vaccinetrial.co.uk/phase-iiiii-trial-explained
[6] https://en.wikipedia.org/wiki/COVID-19_vaccine
[7] "COVID-19 vaccine development pipeline (Refresh URL to update)". Vaccine Centre, London School of Hygiene and Tropical Medicine. 11 December 2020. Retrieved 11 December 2020. Somewhat confusing, but worth the work to understand what's provided if you want detail.
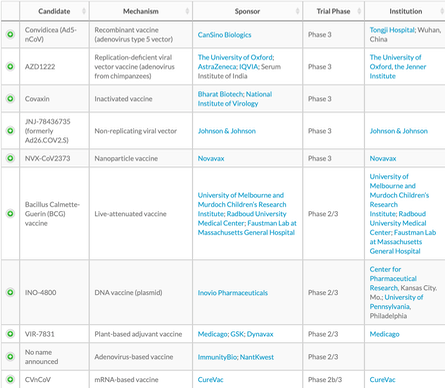
[9] https://www.nytimes.com/interactive/2020/science/coronavirus-vaccine-tracker.html#beijing NY Times round up on the same topic as this page. I've opted for this source's tables, as they are updated more often. ----> Last NYT update 24th Jan. ---->
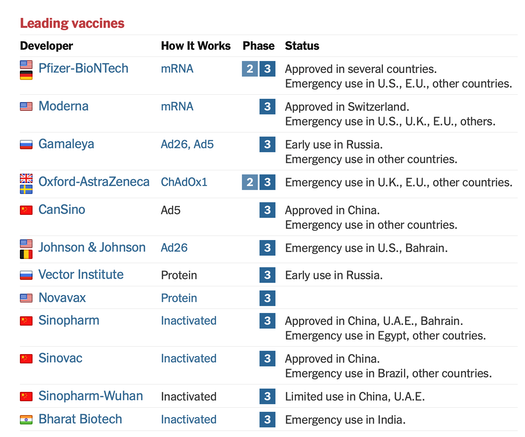
Vaccines under construction: approved here and phase 3 below
In order of appearance (in the media, or if you prefer, as noticed by me);
https://www.raps.org/news-and-articles/news-articles/2020/3/covid-19-vaccine-tracker
https://www.who.int/publications/m/item/draft-landscape-of-covid-19-candidate-vaccines
Pfizer/BioNTech this is the one that has to be kept very cold, like -70ºC. Approved in the UK EU, 20201221 and the UK, earlier. 95% effective. mRNA type vaccine, which is new. Developed in the UK, Germany and mostly made in Belgium. Check this. BBC report.
Moderna/NIAID, 95% effective in trials. Same mRNA approach, 5M doses ordered for UK. Kept at -20ºC. Approved in Canada 20201223, and US, later.
Oxford / Astra Zeneca either 70% or 90% effective, depending on delivery (so 90%, since obviously one will choose the more effective route). 100M UK doses ordered. AZ has this wonderful policy to supply to poor countries at cost. Long may they succeed. UK approved this on 20201230. EU approved Jan29th for use with all over 18.
Russian Sputnik V, same approach as Oxford, 92% effective
Janssen has reached the mass testing stage. Adenovirus approach as Gamaleya, below). Jan29th moved to UK approval.
Novovax recombinant SARS nanoparticle vaccine with adjuvenant. Jan28th moved to UK approval.
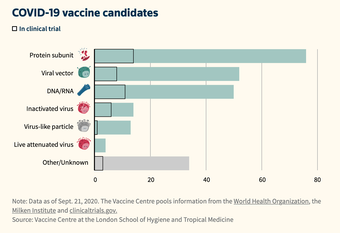
Wuhan, Sinopharm, Gamaleya as in the tables hereabouts. There are, as the WHO extract shows, 52 in clinical evaluation.
Target: herd immunity is around the 70% mark of the global population. Which I reckon means we need to have inoculated 80% at 90% effectiveness. That is a huge target, bearing in mind the turnover of population. Just maintaining a position is a huge undertaking, let alone reaching the target. We have yet to discover the period at which boosters will be required. If this is more frequent than annually we have a whole new class of difficulty, possibly culture-changing. Pun intended.
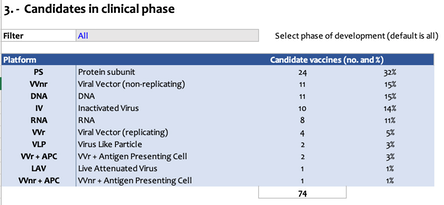
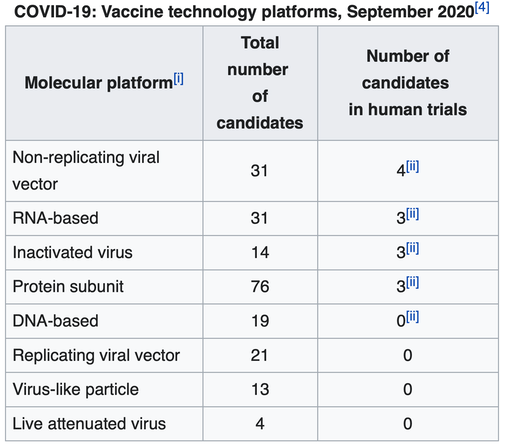
Take WHO link to https://www.who.int/publications/m/item/draft-landscape-of-covid-19-candidate-vaccines, Download 12-page pdf. Some of page 1 reproduced above. This is updated frequently. 20201222 update says 172 in pre-clinical development, a further 61 in clinical development. This is a spreadsheet that is updated quite often. Sample table here -->.
This paper from 2013 suggests that only 22% of the initiatives were forecasted in 1996 to successfully reach the market after 10 years of development, and that the average vaccine, taken from the preclinical phase, requires a development timeline of 10.71 years and has a market entry probability of 6%. Which might suggest that of the 52, we could expect 3 to survive or for 11 to survive. Taking the more optimistic number (applying the 22% figure) then we should be able to look at some probabilities, which implies a whole extra page in the Maths section. For example, the probability we have only up to two successful vaccines from 11 reaching clinical trials is .78¹¹+11(.78)¹⁰(.22) + 55 (.78)⁹(.22)² = .551, that is, P(X≥3)=0.551
Similarly, that only up to 3 of the 52 reach completion at 6% success is 0.62, as shown here;
P(X≤3|X~Bin(52,0.06)) = 0.94⁵² + 52(0.94)⁵¹(0.06) + 1326(0.94)⁵⁰(0.06)² + 22100(0.94)⁴⁹(0.06)³ = 0.620
So the P(X>3) of more than 3 succeeding is 1-that = 0.38 and of more than two p(X≥3) succeeding is [...] 0.610
20201222 Sharon Peacock on the new variant. Good stuff.
The intended vaccination process within the UK aims to maximise the number of people covered. So instead of delivering two jabs at the optimum / expected interval of three weeks, that interval is increased to 12 weeks. This means that far more people—like twice as many—can be jabbed in the same period and, provided efficacy is over 50%, this is a win. Efficacy is thought to be in excess of 70% over this 12-week interval, so this is a significant win. Presumably at 12 weeks the effort goes into second jabs so that the bigger number of who has been declared as at-risk is boosted to much longer-term cover. Meanwhile the under-16s are not included in the licensing and the 16-50 group are considered not at risk. The impetus is driven by the understanding that the vaccine is very good at preventing the virus from serious illness, though we're not so very sure about infection rates. At 2M jabs delivered a week and starting at that volume from mid-Jan, we have 13 million 1st wave to include, so probably late February, with antibody counts significant three weeks later, say mid-March. The second round jabs for that group start mid-April (or sooner), so the 50-70 age-group (second wave along with non-medical key workers) may be jabbed at for the maybe six weeks between March and the mid-April moment. Secondary jabs for the second wave begin in mid-July, so that the third wave, everybody else that wants a jab, runs whenever there is spare capacity. We expect the 2M per week to rise, perhaps as high as twice that. Of course, there comes a point at which demand from elsewhere takes precedence, so it seems to me quite likely that those considered at low risk continue to be uninoculated. It is also possible that by say June we have a wider range of working approved vaccines (not just in the UK, which produces approval relatively quickly) to choose from. What we still don't have is a good supply chain. I see this position changing; politically the need to be able to generate vaccine within our borders has been something I first identified in the March essay. I wrote then that Apparently, Britain has no in-country facilities for generating vaccine stock. So that is poor security of supply, which is something we will see criticised around the world as the year goes by. See link (in the line above, August 2008) for comment on public sector vaccine manufacturing. It is apparent now that we have vaccine made by Astra Zeneca and in Oxford and Cobra Biologics in Keele; from bulk manufacture there is a pause while batches are tested for quality, something of a hold-up currently, then there is what is called 'filling and finishing', putting bulk vaccine into vials and labelling, which takes place in Wrexham and where we identify a mass shortage of the little glass bottles. I read that we have a new facility, VMICuk, under construction at Harwell, south of Oxford. Perhaps someone was reading my stuff, after all; more probable to have been like minds running in parallel. VMIC may even open in 2021. “We repurposed two facilities – one in Oxford, with Oxford Biomedica, and the other one in Cobra Biologics in Keele and they have been manufacturing AstraZeneca vaccine for some months now. And it’s being finished in a company called Wockhart in North Wales,” [...] said Ian McCubbin, manufacturing lead for the Vaccine Taskforce.
Pfizer manufacture: Through its existing mRNA production sites in Mainz and Idar-Oberstein, Germany, BioNTech is able to produce mRNA for commercial supply after having already produced the vaccine candidate doses for the clinical trials. BioNTech will also increase its manufacturing capacity in 2021, once a third site in Germany will start manufacturing to provide further capacities for a global supply of the potential vaccine. Critical to distribution in the U.K. will be Pfizer’s manufacturing site in Puurs, Belgium, one of Pfizer’s largest sterile injectable sites. The Puurs site is being used primarily for European supply but will also serve as back up supply to Kalamazoo, Michigan, for the U.S. market. source.
The priority list for who is to be vaccinated is here, in quite a bit of detail. This page is updated, too.
1. residents in a care home for older adults and their carers
2. all those 80 years of age and over and frontline health and social care workers
3. all those 75 years of age and over
4. all those 70 years of age and over and clinically extremely vulnerable individuals[footnote 1] UK target to complete these (1-4) by mid-February 2021
5. all those 65 years of age and over
6. all individuals aged 16 years [footnote 2] to 64 years with underlying health conditions which put them at higher risk of serious disease and mortality[footnote 3]
7. all those 60 years of age and over
8. all those 55 years of age and over
9. all those 50 years of age and over
Where you have a group that thinks they are more at risk (teachers, for example) the evidence as collected and analysed says that in practice there ç no more deaths within this group than if the grouping was something different. That is not illnesses, nor is it a reflection of the consequences of there being a significant proportion of due to sickness or isolation (one thinks of the third of NHS workers off for that cause and its consequences). The thinking is that this is a health issue, which includes no economic attributes, which is how things like school are viewed. So all the detractors are demanding that there be a political decision as to who to protect. The answer, to date, is that we protect those working in trying to reduce death.
Update on when for inoculations with what I think are reasonable dates not politically optimistic ones. 210118.
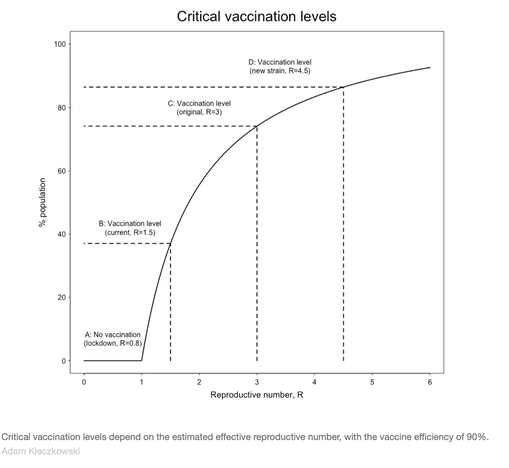
Update 210118 on what herd immunity means, explaining why 70-75% was the original critical point , but now another 10% is more like the minimum value. the helpful graph shows how the modelling balances restriction on movement / socialisation (in effect where we allow R to be) against population inoculated. Go the wrong side of the line and we're off (off work, back into the repeating cycle and in lockdown) all over again. If you come across lower figures for herd immunity, that's because you have to factor in the efficacy of the jab, which always moves the herd immunity target upwards. The article points out—as I've already observed—that reaching a 90% point in any population is quite difficult, while I say maintaining that level is also hard work. So we need to budget for that maintenance work (and you can bet we haven't).
Update from The Conversation, 20210121. People should be realistic in their expectations....the government is aiming to have delivered the first dose to every UK adult by September....History tells us that mass vaccination campaigns tend to be shambolic.... For lower-income countries[..] widespread coverage is likely to be years away.
The race to protect the most vulnerable continues. But if the virus is to be eradicated, testing and social distancing will need to continue to be part of the plan, alongside vaccines.
The UK has ordered, in expected order of arrival if at all:
100M of the Oxford-AstraZeneca, 40M of the Pfizer-BioNTech, 17M of the Moderna, 60M of the Novavax, 30M of the Janssen (Johnson&Johnson), 100M of Valneva upped from 60M on 1st Feb), 60M of GSK (with Sanofi Pasteur). BBC report.

Early Feb 2021: In terms of security of supply, much improved from a year ago, the general position is quite difficult to sort out. Valneva reads as French but is made in Scotland, perhaps among other places. Some of delivery in expected occur in late 2021. AstraZeneca is made in England (mainly) and in Belgium. We might well expect that the Belgian site will provide the majority of the EU supply. Pfizer has many sites and EU/UK supply will dwindle, I expect, as soon as it is approved by the FDA. Moderna is based in Massachusetts and the bulk of its output will stay in the USA, at least for the forseeable future; some may arrive in the UK in April; the EU ordered this in volume (160M doses) and is expecting delivery in February. Novavax is also American, but has a manufacturing facility in Stockton-on-Tees (in England) close to completion and delivery may begin in May along with MHRA approval. Janssen is in much the same position but based in Belgium, although Janssen is part of the much larger Johnson & Johnson and is special for only needing a single dose (as yet, Phase 3 trials with two doses are in progress); if approved it may arrive in late summer or the autumn. GSK-Sanofi is going a little more slowly and may arrive in late 2021 (it's not working well with the older groups). GSK is based in London, so one assumes there are some manufacturing facilities within these borders and many elsewhere. Most vaccines are made in Belgium. UK supply 2021 (inset diagram from this last FT link).
DJS 20210202
One question, answered: Why are vaccines given in the upper arm?
Our staff writer Katherine J. Wu, who recently wrote about why the vaccine’s second shot can rile up the immune system, has an answer:
Targeting shots to the deltoid muscle hits a perfect sweet spot for vaccines, distributing their contents quickly, without diluting or destroying the important ingredients. Muscles are rife with blood vessels, which disperse the vaccine’s contents throughout the body and provide a conduit for immune cells to move back and forth from the injection site. They are also naturally chock full of “messenger” immune cells, which can quickly grab hold of the bits of the vaccine that resemble the coronavirus and carry them to the rest of the immune system. This baton pass kick-starts the production of antibodies and other disease-fighting molecules and cells.
Injecting a vaccine directly into the blood would water it down too quickly, depriving immune cells of the opportunity to learn from it. Spiking it into a fattier tissue, such as the buttocks, would slow the process down too much because fat isn’t laced with as many blood vessels, and is also lacking in many of those crucial messenger cells.
Savor that upper-arm shot: It might ache for a bit, but only because your immune cells are already hard at work. The Atlantic header mail, 20210212.
Personal: I'm in tier 5, 65-70 age group, and went to my local health centre to be jabbed on Sat13th Feb. I'm not the first in the family: my SiL (son-in law, for those who don't use TLAs) is an optician and was jabbed several weeks ago as being medical personnel. The boss, who is a teacher, thinks she is a very long way from inoculation. I'll record that moment on here.
Related Pages: (faulty links updated 20201202)
Essay 291 - Effects of an outbreak what it says, effects, but some description of what we have (and not)
Essay 293 - Covid-19 charts charts published daily reflecting concerns and issues.
Essay 295 Long-term Distancing
Coronavirus (Y10+) modelling problems
Epidemics more general theory
Infectious disease looking at the 2020 problem, particularly effects of the reproduction number changing.
Essay 298 Covid Consequences Surprisingly prescient, considering when it was written.
Essay 304 Covid Disparities A report on the report, including what it doesn't say.
Essay 311 Covid in August International charts updated
Essay 316 Covid in September European comparison charts updated
Viruses are very small Worth reading, I think. (But I would, wouldn't I?)
Essay 318 Covid in October Charts updated through November
Essay 322 Covid in November UK Regional chart and table through Lockdown Two
Essay 325 Covid in December Updated graphs of rate and prevalence, plus US charts.
Essay 328 Vaccine progress This very page
Essay 332 Covid in January Maunderings through the month, very bored.