
 20210706, Sajid Javid (newish Health Sec, UK) tells the HoC about the prognosis (heavy) for the summer covid cases. Read. I understand the political wish to remove all regulation. At the same time I think that this leaves those of us that wish to maintain a higher (than zero) health safety regime in a precarious position every time we mix — at the office, in meeting obligations, anywhere where we have very marginal control of our own position. We continue to have zero progress and no intention to make progress on sick pay provision for those caused to isolate; that means that the incentive to not isolate is exactly as it was a year ago. We have the usual screamers from the sidelines, everyone of them with a glaring blaze of self-interest. Ten day isolation after exposure continues to Aug 16 (in theory, in law). I see little reason why you would continue to use the NHS app (then or now, for that matter) if there is no personal advantage to gain from isolation, but that is a different complaint. Absence from school last week, 641,000. Source. Covid dashboard.
20210706, Sajid Javid (newish Health Sec, UK) tells the HoC about the prognosis (heavy) for the summer covid cases. Read. I understand the political wish to remove all regulation. At the same time I think that this leaves those of us that wish to maintain a higher (than zero) health safety regime in a precarious position every time we mix — at the office, in meeting obligations, anywhere where we have very marginal control of our own position. We continue to have zero progress and no intention to make progress on sick pay provision for those caused to isolate; that means that the incentive to not isolate is exactly as it was a year ago. We have the usual screamers from the sidelines, everyone of them with a glaring blaze of self-interest. Ten day isolation after exposure continues to Aug 16 (in theory, in law). I see little reason why you would continue to use the NHS app (then or now, for that matter) if there is no personal advantage to gain from isolation, but that is a different complaint. Absence from school last week, 641,000. Source. Covid dashboard.
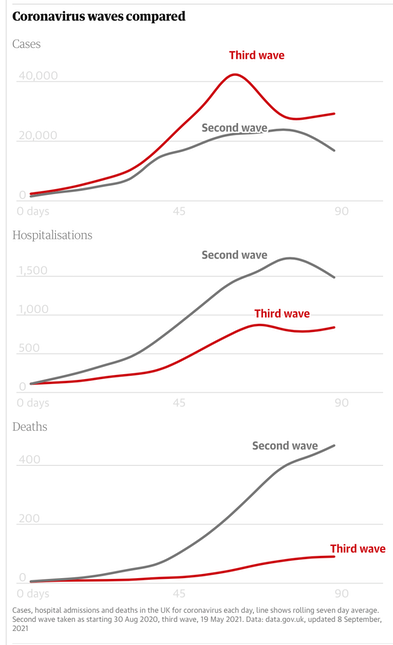
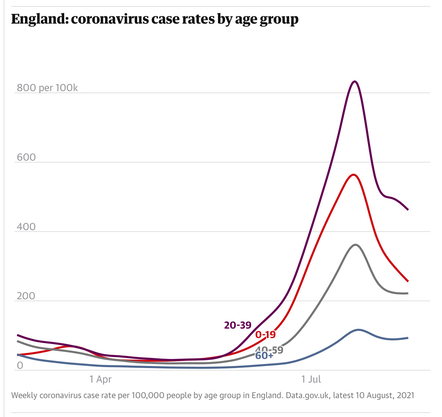
It is the risks attached to the case count that has become very much less clear. Not least, who risk applies to. Hospitalisation (2140 covid cases on 20210704) is less likely. ¹ Current hospital cases divided by new cases today is at a new low of around 7.5% and is a crude if easy measure. Yet a prediction of 100,000 cases puts the NHS back in a position quite similar to a pre-covid winter flu season. See the chart to the right.
It seems to me fairly obvious that the number of people presenting at hospital with covid and already having had two jabs is going to rise. The vaccine is not perfect; the population with no jabs is reducing. What is not clear is what the state of those in hospital is, whether these are folk with underlying issues in similar proportions to what was observed a year earlier, whether there are some obvious clues as to who is more susceptible, even whether what we already think we know is still applicable. As the subtext is 'it's all over' or very nearly so, so the availability of information dries up. But it seems to me that the surge shown immediately to the right is quite sufficient cause to reopen the files and check that what we think we know is actually so.
1 1st wave Apr'20, wave case peak 5,000 with 20,000 peak hospital covid cases, factor of 4. 2nd wave Nov '20, 23,000 and 17,000, factor below 0.75, 3rd wave Jan '21, and 55,000 and 37,000, factor about 0.65. I recognise this is a very crude measure.
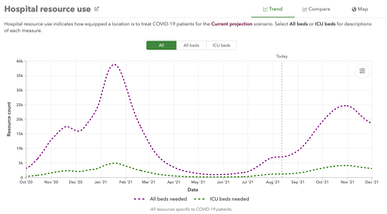
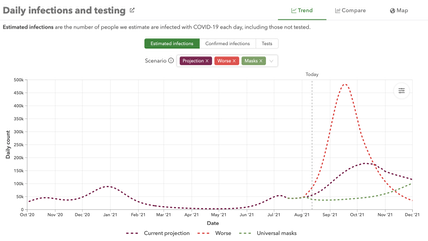
I found a prediction of hospital resource use; the upper line is 'all beds', the lower is ICU demand. To my eye that looks very bad. The chart on the left shows estimated covid infections; the bottom line shows lots (100%) of mask use, the red line a 'worse' case that fits my own image of 'Freedom Day' consequences and school hols and all sorts of suppressed activity bursting into action.
You might look at the same charts for other nations. I looked at Belgium, France, Germany, Spain, and Greece, for all of whom all the lines trend rapidly to the axis. Portugal is predicted much the same behaviour as ourselves; Brazil is forecast a rapid decline a little later; the USA a slight rise. Of the countries that I looked at, the UK stands out as either a source of very different information or a place that the wise would avoid. To coin a phrase, avoid like the plague. 20210707
Charts updated 20210812
__________________
Like many others, I have been comparing covid with influenza. I have done this because 'flu is the disease I know of that is responsible for a similar number of deaths historically and which we treat in much the same way. But it is not the only such disease and I discovered that there are arguments for norovirus to be a better comparator. I barely know what that is, so refer you to this, at The Conversation. ¹. We compared SARS (in Britain) with flu, but also with itself. But in China and Korea, SARS had a far greater effect and (so) their reaction to covid was also more severe. With the visible result that their covid experience has been, in comparison to ours, no big deal at all and I'd compare their experience to something more like the last round of foot-and-mouth in Britain - it affected everyone in terms of restriction, but very few people died though there were business losses (a coarse description for losing your entire herd). Moreover, the far east now has a routine that they have shown works, while Europe, for example, has shown something quite different and one possible result would be that Europeans will have to prove a clean bill of health if visiting the PRC – and I'd understand any push in the Middle Kingdom to close the border to those proven foreign idiots.
The significant issue that I take with the political attitude (as perceived) is that they are okay with anyone and everyone catching covid. Which is, I think, the way we think of the 'flu. We vaccinate only those who are particularly prone to complications and treat people with severe side-effects, such as pneumonia. Otherwise, people are left to go about their business. I disagree with this policy, and that is what has been bothering me of late, that I'm not at all content to have 'had' covid, mostly because there is an unspecified risk of long-term effects, which therefore make these diseases (covid and 'flu) non-equivalents. One in ten who has had covid is still experiencing symptoms 12 weeks later. See. One measure that stands is that, in trying to cope with covid, we effectively had a winter without flu. Therefore it is clear that (i) covid is more infectious and (ii) we are capable of reducing flu by far more than we have actually achieved. We must not lose sight of the fact that flu is a disease that we already inoculate against, and though we do tend to push the flu jab at those deemed vulnerable we also make it available to practically anyone who wants it.
Norovirus, says Sarah Pitt in the linked article, stands comparison with coronavirus. It too can be asymptomatic in some people, and mutates rapidly – different strains of norovirus have been found circulating around the same hospital during one season. In fact, as it spreads around, norovirus sometimes changes so much that standard testing kits can’t recognise versions of it that have evolved. With norovirus, we keep people with the infection away from others. We ask parents whose children have symptoms to keep them off school. And in hospitals and care homes, patients with norovirus are nursed separately from others, staff use PPE for protection, and surfaces are deep cleaned. Handling COVID-19 in the future should be more interventionist like this. It should be more akin to living with norovirus than the flu.
The article stops at this point when I'd like suggestions as to sensible long-term behaviour at an individual and a collective level. I promise to myself that I will maintain higher standards of washing, I will continue to attempt social distancing and I will keep masks on hand for occasions where distancing fails (plural because while I only need one, I need that essential available in many circumstances). There are some activities common to many that I already do not do and a few I have recently decided will not occur. I suspect I have taken my last air flight and, thanks to Brexit, I may never cross the border again; already I have allowed my passport to lapse. I do not and did not support Brexit; I liked being a European and I visited often. But it doesn't take much in terms of increased hassle to cause me to not bother and, in a world in which sustainability is an issue, I don't feel the need for travel, though I did often appreciate that travel does indeed broaden the mind; I will merely have to find other ways to achieve that breadth.
__________________
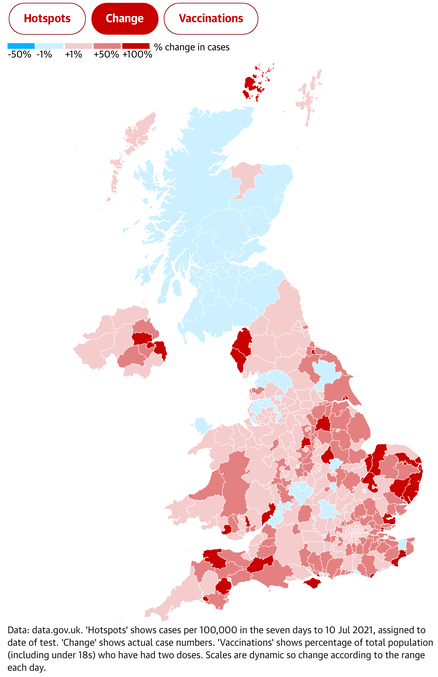
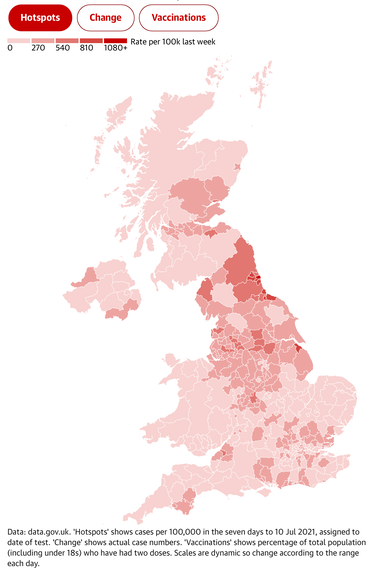
Case count figures continue to rise. The sport this weekend doesn't assist any reduction in the acceleration. Hotspots to the right, change on the left.
1 Be aware that I criticise The Conversation for its strapline 'academic rigour, journalistic flair' because it fails all the tests of academic rigour (that my daughter keeps me up to speed on, most weeks), but I would accept Guardian-level links to (some of) the background papers that inform the opinions that the authors so happily proffer without what I consider adequate explanation. Which last is, presumably what 'flair' is, getting away with ducking conventions such as how arguments are put together. I cannot even successfully write to The Con to let them know directly. This piece did what I want and connects with sources.
DJS 20210711
Happy birthday, boss
undated charts updated 20210716 and 20210811 (another family birthday)
Added in August: Blackpool case rate at just under 500 phut, Lincoln and Exeter over 600phut week to Aug 6th. Hospitalisation may have levelled off at around 6000 on any day. Guardian dashboard. Vaccination has passed 75% of all adults having two jabs, but the rate of jabbing has dropped steadily since June. The sensitivity of 'the app' that pings you if you've been close to an infected person has been reset so that it is less sensitive, giving us the new word 'pingdemic'. Allegedly many simply ditched the app (I never loaded it, but then I don't use a phone much at all). 20210812
I updated a chart in early September in lieu of repetition later.