
 I suspect that the UK has declared covid to be, basically, over. I have therefore titled this as if it is and I will retitle the page as necessary. I expect to renew this page several times, up to the moment at which updates to the several reference pages cease being made available.
I suspect that the UK has declared covid to be, basically, over. I have therefore titled this as if it is and I will retitle the page as necessary. I expect to renew this page several times, up to the moment at which updates to the several reference pages cease being made available.
https://coronavirus.data.gov.uk/ dashboard for the date, 20220102... The link is going to be more up to date than my screen dump.
reference link, for updates on 'variants of concern': https://www.gov.uk/government/publications/investigation-of-sars-cov-2-variants-of-concern-routine-variant-data-updatehttps://www.gov.uk/government/publications/investigation-of-sars-cov-2-variants-of-concern-routine-variant-data-update is the header page and this is update 13 for the end of 2021; https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1018456/Variants_of_Concern_Variant_Data_Update_13__21_09_16.pdf
Here's a link to the latest ONS survey, perhaps the only reliable measure remaining. If there is newer still, the linked page points at the newer file.
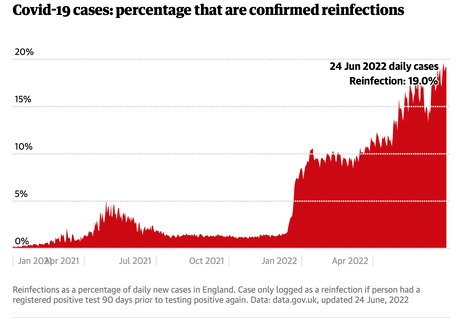
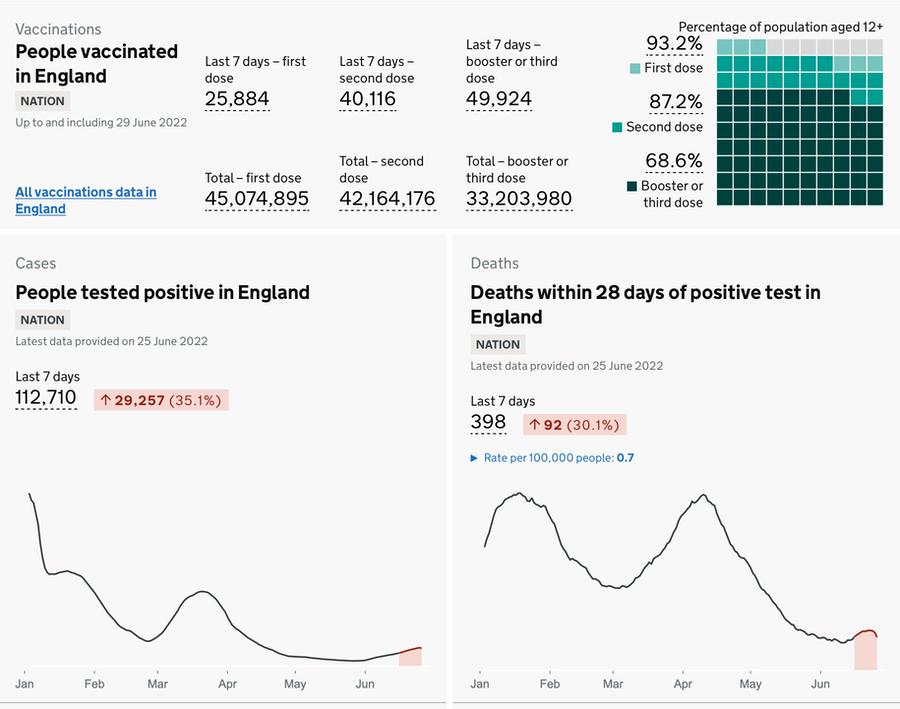
Go to Covid dashboard @ Guardian for the current position. Compared to the January page, I have added the (red) reinfection graph.
DJS 20220220
... with edits and updates done 18th, then ......
I reported on (gov.uk coronavirus site) vaccination take-up for where I live, 2nd Jan. Utterly pathetic: 1st dose 72%, 2nd dose 64%, booster/3rd 43% - that's at MSOA level. At UTLA, which is Blackpool, 80%, 73% and 53%, which is still awful, indicating a whole 20% who haven't taken the first step towards vaccination. I despair at my fellow man. [1] At February the immediate, MSOA, figures are 73.0%, 65.6% and 47.3%, a very slight improvement while the UTLA figures are 80.7%, 74.7% and 57.3%, again barely shifted. I conclude that those who have so far refused to be vaccinated conclude that they can continue to be in that state, while those who feel safer jabbed have continued to collect their third/booster. I expect, then that the general attitude will become very much as it is for the influenza jab.
https://bmcpublichealth.biomedcentral.com/articles/10.1186/s12889-021-11736-2 is a report on just that, take-up of the 'flu jab. This hovers around 50%, where the ambition was to have it around 75% within at-risk groups The phrase herd immunity applies but was rarely seen (twice) in my read of this. I am not saying that half the population gets jabbed; only that half of those offered the jab (i.e., in the at-risk groups) take it up. Here's a sample (on the right) of the detail available (see the National tab); I read it as the over 65s responding well at 80% uptake, while the 50-65s not at risk have a 25% uptake, dragging the mean of that age-group down to 38% in the season 21/22 (Sep-Dec 2021). Those between age 3 and age 50 are not offered a jab (except when there are jabs available and unused). I didn't find a count or report of the numbers of jabs purchased. The ambition is to vaccinate the at-risk groups, especially the elderly (me and worse) as there is an obvious correlation between age, flu and hospitalisation due to the severity of the illness.
I am expecting covid to be added to the list of respiratory diseases we attempt to fight against. That says nothing about long covid, which is what I continue to see as the particular threat. I have often thought that in war there is an argument that injuries are more useful than deaths, because injuries soak up loads of resources of those (enemy) one has caused to be injured. Horrid though the thought is, we spend relatively few resources in coping with the dead. So there is value in spending resources so that we reduce and avoid as much as possible the extensive use of resource that is incurred when we try quite hard to prevent deaths from occurring. Just from an accountant's paper-pushing viewpoint, which I see as quite likely what happens at a state level, we therefore are wise if we find ways to reduce the numbers requiring extensive and expensive treatment. Few states can ever get away with permitting deaths to occur, so we assume that the nation state will try to keep people from dying. Therefore the sensible effort will be directed to reducing those identified as at-risk. We have seen this close up and personal through 2020 and 2021 and I would like to think that we have learned from this. However, the state of our media is such that I am far from sure that we have learned the same lesson (at all). There yet may be consequences in regulatory terms (such as being required to have various vaccinations to be employed).
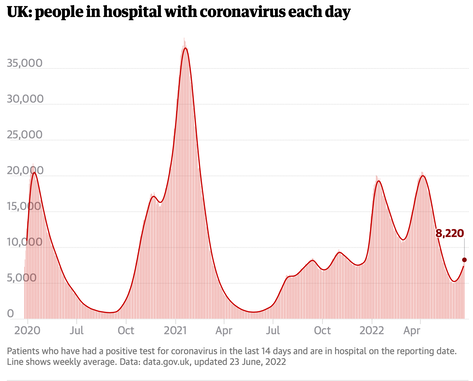
Update, 20220502. I added the hospitalisation chart, because I see these figures as alarmingly high and largely unreported. Anything that causes in excess of 10k people to be in hospital should be, one would think, a cause for concern and concerted action. One wonders why we would choose to simply ignore this. Further, bearing in mind that we have learned to expect waves of infection to occur in what we call winter, one wonders also how we have allowed this to happen in spring. I rather assume that a spell of warmer weather couple with the Easter holiday will be given as excuse/reason. I also assume that we have a consensus opinion (perhaps originating in parliament) that we want this to be over, so therefore we simply declare it to be so. Thus we have the herd immunity assumption that we so abused two years ago. I note that we are no nearer having a decent official sick pay arrangement and we're largely back to the original position ("I have a wee cough, can I have a week off?"). Fuss in the press over various large employers actually following gov't guidelines about declarations and testing for covid, so that we';re back to presenteeism (where you cannot afford to be off work, so you go in, knowingly likely to infect your colleagues).
So covid is declared over simply because some of us wish it to be so. Move along, nothing to see here. Given the chronic shortage of money funding all sorts of public services including health and council services, we should therefore expect that long covid will have many reports showing massive underfunding, with only token gestures towards assistance.
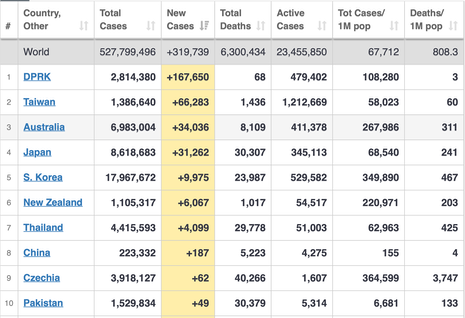
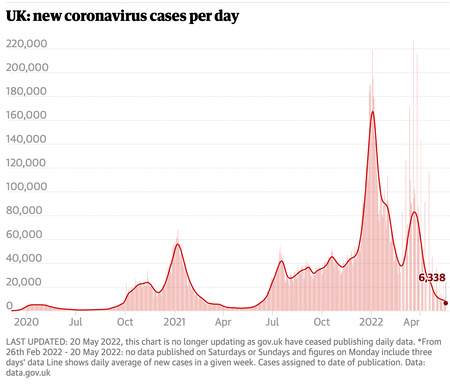
Update 20220523. More of the same, actually. If we don't test the public, how would we know anything about the situation? The ONS latest, this week, referring to the end of April, says prevalence is 1 in 55 in England (Sco 45, Wal 40, NI 60) which is still declining (which is good). If there is anything trending upwards it is in the very young and the 25-34 groups. I recommend Fig 5 for a feel for how the figures are dropping. The media are making a lot more fuss over monkey pox, count of 20 cases, than covid, well over a million current cases. We have suitable vaccines and the monkey pox is said to be relatively difficult to pass on. That link, CDC, does not indicate so. Given that one suspects many of us have developed new habits such as better hand-washing and still frequent use of sanitiser, I'd expect transmission to be confined to social groups that ignore such precautions. Of course, since yet again we're looking at a virus transmitted by airborne droplets, this is another threat and ought to be treated as 'more of the same' not remarkably different. Meanwhile, North Korea seems to be having a covid disaster at the moment. Whether this is from accepting that there is a problem and so discovering the numbers (rather than ignoring them), we cannot know. I've inset today's chart from worldometers, sorted by new cases. But if you don't test, you have no idea what the position is.
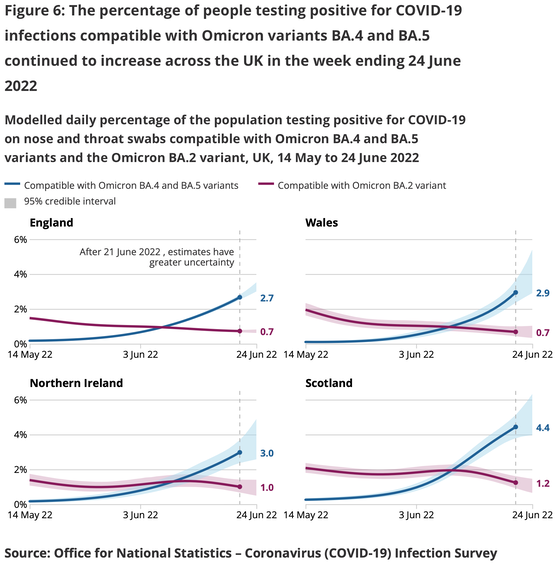
Update 20220621 The ONS May report says prevalence (positivity, irrespective of symptoms) moved to 1 in 50 for England (Sco 30, Wal 45, NI 45). This means we have considerably more people testing positive. Omicrom variants BA.4 and BA.5 are declareed to be significant and are, at the time of writing, becoming the dominant strain in each of the four nations. I am a little surprised we don't have a push for another round of vaccinations. I note a jump in hospital admissions. This in the context of sudden recognition of cost of living crisis, increasing inflation and this recognition is bringing a round of strikes.
DJS 20220220
(much actually written on the 18th, but it's too nice a date to not use it)
Charts updated, 20220315, 20220502, 20220523, 0701....
The July 1st update added this infection survey from the latest ONS review. It shows the switch from BA.2 Omicron to BA4&5, such that the newwer vriant became dominant in mid-June.
The graphic for hotspots on the Guardian site is effectively dead since the gov.uk site is no longer publishing data (as of the start of June). Instead, look at the ONS survey Figure 3.
I am still expecting that a vaccine booster, quite different from listening to BoJo on any topic, will be offerred in the early autumn. No doubt that will be seen by me (over 65) as a command to attend and by the wife (full-time teacher) as something she ought to have if she can find it on offer. which for both of us might well be simultaneous with the next 'flu jab; we know they can be given at the same time.